After four years selling to pharma, co-founders Robert DiFazio and Juliana Hilliard are adding a new line of business: their own drugs.

Plates of organoids being automatically fed to grow and develop into replicas of human lymph nodes. [Photo credit: Parallel Bio]
“We put it in our system and showed the exact same response,” says Robert DiFazio, co-founder of Parallel Bio. Its human organoid platform predicted, retrospectively, the failure that animal models missed entirely.
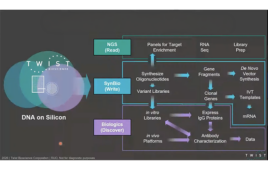
Parallel Bio, founded in 2021, builds human immune organoids, functioning in-vitro replicas of lymph nodes that can predict how drugs will perform in people before they reach clinical trials. The company has signed on eight pharmaceutical partners to test drugs using its “Clinical Trial in a Dish” platform. DiFazio and co-founder Juliana Hilliard are now exploring in-house drug development, with an eye toward filing their own INDs.
The company has collected validation data that mirrors real-world outcomes. In tests using a large number of donors, their organoid system showed the rabies post-exposure vaccine, which is nearly 100% effective when administered promptly, working universally across samples. The flu vaccine, which hovers around 40-60% effectiveness depending on the year and strain, worked in roughly 60% of their donors. “But that allows you to pick those 40% of people and ask what’s different about them,” DiFazio says.
The company is building validated disease models across cancer and autoimmune conditions, with plans to expand its portfolio by mid-year.

Parallel Bio co-founders Juliana Hilliard (left) and Robert DiFazio. Photo: Parallel Bio
The Status Quo
Deloitte’s 2025 analysis estimates average R&D cost per late-stage asset at roughly $2.3 billion, with development timelines from Phase 1 to filing exceeding 100 months. Separately, clinical trial analyses suggest only about 10-14% of drugs entering Phase 1 reach approval. For oncology, it’s closer to 3.4%. In the latter case, the odds are not much better than betting on a single number in roulette.
Why Pharma TENDS TO BE CONSERVATIVE WITH TECH
“Their patents are starting to expire, so they’re going to start acquiring new assets. If they have 20 years left on a patent, they’re not going to invest in new technologies. That’s how they work.” —Hilliard
The Realization
“This has been a four-year process of realizing the emperor has no clothes.” —DiFazio on industry inertia
The Proof Point
TGN 1412 was safe in mice, safe in monkeys, and almost killed six people in Phase 1. Parallel Bio’s organoid system showed the same deadly immune response. It would have stopped the drug before it reached humans, DiFazio says.
The Pivot
“If we actually want to have the impact we hope to have, we need to start making our own drugs.” —Hilliard
The 50-Year Vision
“We will not be testing in animals, and I don’t think we’ll be testing in humans either. All of drug discovery will be done virtually.” —DiFazio
During a safety project with one Fortune 500 partner, the company asked Parallel Bio to use a specific molecule as a benchmark. It didn’t produce the expected response in their human system. When DiFazio raised the issue, the partner’s team pushed back: the molecule should be highly immunostimulatory. The data showed it clearly.
“I said, ‘The papers you sent. This is mouse data,'” DiFazio recalls. “They said, ‘Yeah.’ I said, ‘We’re testing it in a human system. I would actually be shocked if it had this effect in humans.’ They said, ‘But the data…’ I said, ‘Data in mice.'”
And mice are just the start. Men are more likely to die from infectious diseases; women are more likely to develop autoimmune conditions, a divergence driven partly by sex hormones that directly regulate immune function. Yet preclinical testing still relies heavily on single-sex inbred mice, collapsing human diversity into a single genetic line. “It’s ignoring facts,” DiFazio says. “It’s the reason medicine doesn’t work for everyone.”
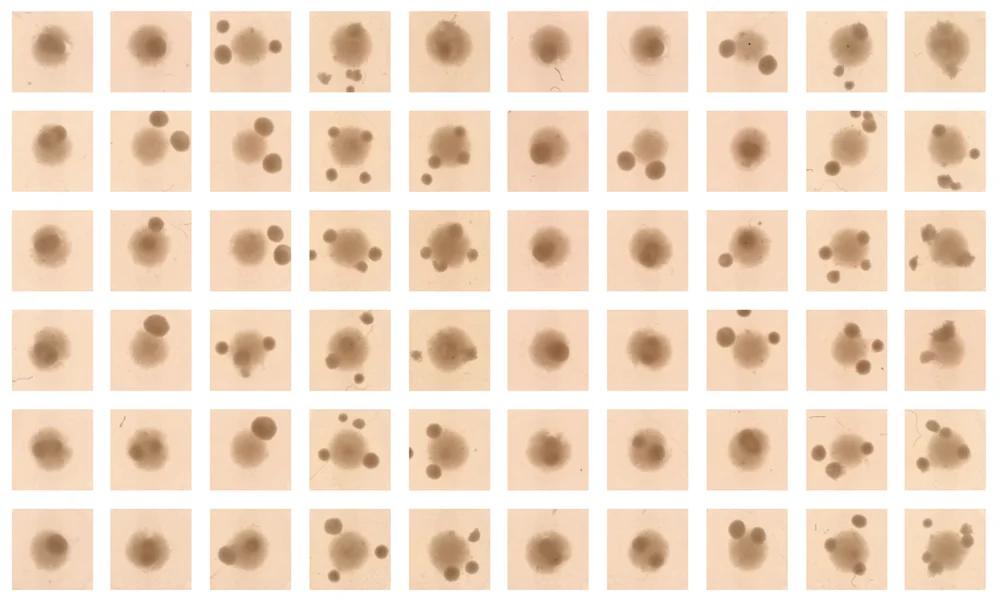
A plate of organoids after being treated with various doses of a drug for testing using Parallel Bio’s Clinical Trial in a Dish. [Photo credit: Parallel Bio]
* * *
The FDA may be catching up. The Senate unanimously passed FDA Modernization 3.0 in December 2025; if the House follows, organoid data could support IND filings, a fundamental change in how drugs reach clinical trials.
Then there’s the question of who gets represented. Multiple myeloma disproportionately affects Black people and men. In one clinical trial DiFazio cited, Black participants made up 4% of the study population. “They should have been the entire trial,” he says. “It was inverted.” Another trial included zero Pacific Islanders. These aren’t edge cases; they’re the norm. And behind the statistics: an estimated 100 million mice and rats used annually in U.S. labs alone for research that often fails to translate.
While there has been considerable hype surrounding AI in pharma in recent years, DiFazio is skeptical of silver-bullet framing. For one thing, it isn’t always clear how well the training data is aligned with a given pharmaceutical challenge. “Garbage in, garbage out,” he says. “That’s my biggest criticism of AI right now.” And AI maturity in pharma, as it is in other sectors, is uneven. Companies talk about implementing AI while still siloing data in Microsoft Excel. “Do I think the future will be a digital model of human biology? Absolutely. But the most important thing is: what are the actual data you’re putting in?”
* * *
Ask a patient what that looks like in practice. DiFazio worked on one autoimmune disease at Stanford where the standard protocol upon diagnosis was: “We’re going to try this and see what happens.” The first-line drug works 60-70% of the time. If it doesn’t, doctors switch to another. Then another. The same trial-and-error plays out for antidepressants, chronic pain, countless cancers.
Hilliard and DiFazio see a different potential future. Create organoids from a patient’s own cells. Test every relevant drug, even combinations, on a model of that specific person before they take anything. “Will it work? How long will it work? Which drug would be the best?” DiFazio says. Not a drug tested on a representative population that doesn’t represent you. A drug tested on you.
“I can’t tell you when,” DiFazio says. “But 50 years from now, we will not be testing in animals, and I don’t think we’ll be testing in humans either. All of drug discovery will be done virtually.” The whole process, a year instead of 10.
“We’re just going to bypass all of that,” Hilliard says, “by going directly into diverse human systems, directly into patients.”