[Robeauté]
The Paris startup closed a £23 million Series A round in January 2025 to advance the robot from animal studies into clinical-grade hardware. With “dozens of patents” already on file and a headquarters steps from the city’s life-science cluster, Robeauté claims to be building a platform that can “plug in” new instruments as procedures evolve.
“We’re building what we call a brain gardener, a microrobot that can prune, replant, stimulate growth, and tend to a pathological brain from within,” said Joana Cartocci, Robeauté’s co-founder, at the LSI Europe ‘24 Emerging Medtech Summit in Sintra, Portugal.
As of early 2025, Robeauté is still in preclinical studies although human trials are slated for 2026.
Anatomy of a millimeter-scale machine
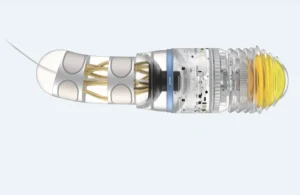
The device measures 1 to 2 millimeters in diameter and only a few millimeters long, small enough to fit through a burr hole no wider than the shaft of a pencil lead. At the point of entry, surgeons need an opening of just 1 to 2 millimeters, roughly one-third the diameter many rigid stereotactic cannulas require. Once inside the parenchyma, the robot advances at about 3 millimeters per minute and can hold its course with an accuracy of roughly half a millimeter.
Microscale rivals such as Bionaut Labs steer untethered bots with external magnets. As of April 2025, Bionaut Labs is also advancing toward initiating human clinical trials for its magnetically guided microrobots, dubbed ‘Bionauts.’
Propulsion without propellers
Traditional catheters rely on either external push-pull motion or hydraulic inflation; both risk compressing delicate tissue. Robeauté instead borrowed from soft robotics. Propulsion via rotating silicone rings exploiting micro-adhesion forces for gentle tissue displacement. The rings expand and contract in sequence, gripping and releasing tissue in a peristaltic manner reminiscent of an earthworm. Because no external fluid is injected, pressure waves and edema are minimized. As the robot potentially shifts to humans, this capability is an important consideration because even submillimeter shifts can affect language or motor control.
The company envisions that neurosurgeons implanting the robot would begin with conventional magnetic resonance imaging to identify a target — for example, the geometric center of a glioma. An AI routine could then calculate a collision-free corridor that bends around vasculature and functional tracts. Robeauté describes a navigation approach using a pre-operative AI-planned path (MRI-based) combined with real-time external ultrasound tracking. Continuous ultrasound feedback would, in theory, update a control loop to issue micro-adjustments to the rings, helping to reduce cumulative error and maintain a 0.5-millimeter accuracy band.